Effects of Flotation REST (Restricted Environmental Stimulation Technique) on Stress Related Muscle Pain: Are 33 flotation sessions more effective than 12 sessions?
Main Article Content
The aim of the study was to investigate whether or not 33 flotation sessions were more effective for stress-related ailments than 12 sessions. Participants were 37 patients, 29 women and 8 men, all diagnosed as having stress-related pain of a muscle tension type. The patients were randomized to one of two conditions: 12 flotation-REST treatments or 33 flotation-REST treatments. Analyses for subjective pain typically indicated that 12 sessions were enough to get considerable improvements and no further improvements were noticed after 33 sessions. A similar pattern was observed concerning the stress-related psychological variables: experienced stress, anxiety, depression, negative affectivity, dispositional optimism, and sleep quality. For blood pressure no effects were observed after 12 sessions, but there was a significant lower level for diastolic blood pressure after 33 sessions. The present study highlighted the importance of finding suitable complementary treatments in order to make further progress after the initial 12 sessions.
Relaxation has become increasingly popular as a pain-relieving intervention (Bood, Sundequist, Kjellgren, Nordström, & Norlander, 2005). It has been suggested that relaxation works by breaking a vicious circle of pain (Linton, 1982). This is in accordance with the neuromatrix theory of pain (Melzack, 2001) which suggests brain mechanisms for chronic pain and also indicates new forms of treatment. Relaxation exercises offer the means to reduce physiological and psychological reactions to stress (Sandlund & Norlander, 2000). Different relaxation techniques often lead to specific psychological and physiological changes labeled the ‘relaxation response’ (Benson, 1975).
In the present study, a floating tank was used to induce the relaxation response (RR). In flotation-REST (Restricted Environmental Stimulation Technique) an individual is placed in a horizontal floating posture and immersed in highly concentrated salt water in an environment (the floating tank) where all incoming stimuli are reduced to the barest minimum during a short period. The flotation-REST technique is not strongly influenced by expectancy-placebo (Norlander, Kjellgren, & Archer, 2001) or by attention-placebo (Bood et al., 2005). Several studies have shown the incidence of positive effects (for a comprehensive review see Bood et al., 2006), such as increased well-being, mild euphoria, increased originality, improved sleep, reduced stress, reduced tension and anxiety, reduced blood pressure and reduced muscle tension. A recent meta-analysis (van Dierendonck & te Nijenhuis, 2005) investigated flotation as a stress-management tool. The study included 25 articles with a total number of 449 participants. The results showed that the flotation technique has positive effects on physiology (e.g., lower blood pressure), well-being, and performance. However, there were some limitations in the original studies (e.g., generally small sample sizes, lack of standardization of the frequency and duration of the sessions) and therefore the available data did not give any information on how many sessions of REST would be desirable for different groups of patients.
Several studies have been performed that apply flotation-REST as a method to alleviate different types of pain conditions (Kjellgren, Sundequist, Norlander, & Archer, 2001). In a series of studies performed by the Human Performance group, Karlstad University, Sweden, it has been shown (e.g., Bood et al., 2006) that a schedule with two periods of two treatments per week for three weeks, separated by a week without treatment, thus giving 12 flotation-REST treatments twice a week during 6 weeks (over a total of 7 weeks), was effective for most of the participants. The positive effects of the flotation-REST therapy typically were maintained four months after treatment. It has not previously been investigated whether or not significantly longer treatment programs (e. g., doubled or tripled) would be more effective than the conventionally used program with 12 sessions. The aim of the present study was to investigate that question.
Method
Participants
Thirty-seven patients, 29 women and 8 men, recruited from the waiting list at the Human Performance Laboratory at Karlstad University, participated in the study. They had been diagnosed by a physician as having stress-related pain, of a muscle tension type. They reported having had pain for an average of 11.14 years (SD = 8.41) and 23 of the patients took analgesics on a regular basis. The average age of the patients was 49.54 years (SD = 8.67). Among the patients, 14 had also received the diagnosis of burn-out depression including symptoms such as fatigue, less energy, loss of self-esteem, problems with organizing daily life, problems with memory and processing new information, problems with sleep, finding that the ailments are not relieved by rest, and feelings of low-spiritedness.
Design
The current study used a three-way split-plot design, where Tests with assessments before and after the flotation sessions constituted the within-subjects factor and where Treatment (i.e., 12 flotation-REST treatments, 33 flotation-REST treatments) and Diagnosis (i. e. nonburn-out patients with stress-related pain, burn-out patients with stress-related pain) constituted the between-subjects factors. The group with 12 treatments comprised 12 patients without burn-out depression and 7 patients with burn-out depression, whereas the group with 33 treatments comprised 11 patients without burn-out depression, and 7 patients with burn-out depression. In the current study there were significantly more women than men, but the men turned out to be quite evenly distributed across conditions, Treatment (5 and 3), and Diagnosis (5 and 3). All participants, irrespective of condition, were treated with flotation-REST during two periods consisting of two treatments per week for three weeks, separated by a week without treatment, thus the group with 12 treatments visited the laboratory twice a week during 6 weeks (over a total of 7 weeks). The other group with 33 treatments visited the laboratory after the initial seven weeks for seven more three-week periods of treatment, with only one session a week (over a total of 35 weeks). The reason for having three-week treatment periods was that female participants could time their flotation treatments around their menstrual cycle. The reason for letting the 33 treatments group float only once a week after the initial two three-week periods was consideration of patient cooperation over such a long time.
Instruments
Flotation tank A flotation tank (Bood et al., 2005; Delfi, www.kikre.com, Varberg, Sweden) measuring 2700 mm × 1500 mm × 1300 mm was used. The depth of liquid (salt water) varied between 200 to 300 mm. The flotation tank was insulated to maintain a constant air and water temperature and to reduce incoming light and noise. The water temperature was maintained at 34.7˚C and was saturated with magnesium sulphate (density: 1.3 g/cm3).
Questionnaire 1 Before the first treatment a questionnaire was provided that estimated each subject’s self-assessed pain: intensity, areas and types, frequency, duration, onset, and treatment, as well as experience/symptoms of other types of complaints. Each subject’s own descriptions of “Most severe pain intensity”, “Normal pain intensity”, and “Sleep quality” were estimated on visual analog scales (0-100) while “Pain frequency” was estimated on a Likert scale (1-5; from rare pain to pain day and night). Additionally, information regarding alcohol and nicotine use was collected.
Questionnaire 2 At a final meeting directly after the treatment weeks of the experimental flotation procedure, the same questions were presented as in Questionnaire 1.
PAI - Pain Area Inventory The PAI test (Bood et al., 2005) consists of two anatomical images of a human being, one frontal and one dorsal. The task of the participants was to indicate and shade with a color pen their areas of pain. A transparent, plastic film is then placed over the colored areas on both figures. Each figure is divided into 833 equal-sized squares (total 1666), and the number of colored squares was calculated. The test was validated (Bood et al.) through comparisons with other instruments measuring total number of pain types, number of connected pain areas − most severe pain intensity, normal pain intensity, and pain frequency − which yielded acceptable values (Standardized item alpha = 0.84, R = 0.70). Test-retest reliability was examined through using a group of patients with pain who completed the PAI on two occasions, seven weeks apart (r = 0.92).
Pain Matcher This test produces magnitude matching with electrical stimulation of the skin, that is, it gives constant current stimulation (Alstergren & Förström, 2003; Cefar Matcher AB, Lund, Sweden). The device is controlled by a microprocessor that provides rectangular pulses with a frequency of 10 Hz and amplitude of 10 mA. The instrument is supposed to give accurate assessments of pain levels experienced by suffering patients. Psychometric investigations indicate excellent reliability scores for pain thresholds (ra between 0.95 – 1.00) but the validity of the instrument’s assessment of pain levels has not been adequately determined (Alstergren & Förström, 2003).
SE - Stress and Energy The SE instrument is a self-estimation instrument concerning individuals’ energy and stress experiences (Kjellberg & Iwanowski, 1989). It consists of two subscales that elucidate the mood levels of the subjects on the dimensions experienced stress and experienced energy. The response alternatives were arranged on six-grade scales, extending from: 0 = not at all, to 5 = very much. The instrument has been validated by analyses from studies focused on occupational burdens and pressures and has test-retest scores of 0.73 to 0.78 (Kjellberg & Iwanowski).
HAD - Hospital Anxiety Depression Scale The HAD is a rating scale for degrees of anxiety and depression, used in various published articles. It was constructed by Zigmond and Snaith (1983), for use with physically ill people. It has since been revised to be used as a rating scale for anxiety and depression. The instrument consists of fourteen statements with four response alternatives (i. e., 0 to 3), ranging from positive to negative or vice versa. Seven statements are related to anxiety and seven to depression.
LOT - Life Orientation Test The LOT (Scheier & Carver, 1985) consists of eight items, plus four filler items. The task of each participant is to decide whether or not he or she is in agreement with each of the items described, on a scale of 0-4, where 0 indicates strongly disagree and 4 indicates strongly agree. The test measures dispositional optimism, defined in terms of generalized outcome expectancies. Parallel Test Reliability is reported to 0.76 and Internal Consistency to 0.76 (Scheier & Carver). LOT is also regarded as having an adequate level of convergent and discriminant validity (Scheier & Carver), as demonstrated by correlation statistics and by using LISREL VI (r = 0.64).
PANAS - Positive Affect and Negative Affect Scales The PANAS-instrument (Watson, Clark, & Tellegen, 1988) assesses the degree of affect, both negative (NA) and positive (PA). The instrument consists of 10 adjectives for the NA-dimension and 10 adjectives for the PA-dimension. In the test manual (Watson et al.), it is postulated that the adjectives describe feelings and mood. The participants were asked to estimate how they had been feeling during the last week. Response alternatives are presented on 5-degree scales ranging from 0 = not at all to 5 = very much.
Procedure
The participants were recruited by asking patients on the waiting list for possible participation in the flotation-REST experiments at the Human Performance Laboratory, Karlstad University, Sweden. The procedure was complete when 40 people agreed to participate in the experiment, and who, according to a nurse, fulfilled the criteria for inclusion. Three individuals at the beginning of the flotation-REST treatment − due to a lack of time − dropped out, thus giving a sample of thirty-seven individuals. Participants had either been referred by their physicians or had responded to announcements calling for individuals suffering from localized muscle tension pain in the neck and shoulder area, with or without temporal headache, associated with myofasical tender points or trigger points.
Each participant’s first contact with the project was an interview with a pain specialist at the initial medical examination where s/he was informed about the project, screened for suitability through questionnaire 1, and underwent a medical examination and a careful pain analysis, including palpation of muscle tone and a neurological examination. During this interview, each participant’s degree of anxiety and depression was assessed using HAD, then the other personality and psychological tests were completed. Among the exclusion criteria were pregnancy or ongoing breast feeding, somatic problems/illnesses requiring other types of treatment, open wounds, manifest psychiatric symptoms, neurological disturbances, whiplash-related disorders, manifest posttraumatic stress disorder, as well as regular treatment with heavy opiate analgesics, and signs of anxiety/fear or discomfort being in a restricted environment.
Following this examination, participants were randomly assigned to either the 12 treatments flotation group or the 33 treatments flotation group. The participants belonging to the 12 treatments group were given flotation treatment during 2 three-week periods (with 2 visits per week), in which each floating session was of 45 minutes’ duration. The number and duration of treatments, that is, twelve over a seven-week period, was chosen from experiences which we had gained from earlier treatments of patients. The participants belonging to the 33 treatments group were first given exactly the same treatment (i.e., 2 three-week periods with 2 visits per week) and after that they participated in 7 additional three-week periods with one visit per week. With regard to the second between-subjects variable of the study, our own previous experience was already available suggesting that approximately one-third to half of the patients with stress-related pain from muscular tension who seek treatment are also diagnosed with burn-out depression. Thus, no further grouping of patients was carried out.
Three days (or 72 hours) after the final treatment session participants attended a final consultation and follow-up discussion, at which time they completed Questionnaire 2 and the psychological tests. All the patients described in the present study completed the whole course of treatment (i.e. twelve sessions or thirty-three sessions).
Results
Pain Measurements
A three-way mixed Pillais’ MANOVA was carried out with Tests (before, after) as the within-subjects factor and Treatment (12 treatments, 33 treatments) and Diagnosis (nonburn-out patients, burn-out patients) as between-subjects factors, and with the number of different ways of measuring subjective pain (i. e., lower pain threshold, upper pain threshold, the PAI, number of comprehensive pain areas, most severe pain intensity, normal pain intensity and pain frequency) as the dependent variables. The analysis yielded significant effects for Tests (p < 0.001, Eta2 = 0.74, power > 0.99), for Diagnosis (p = 0.028, Eta2 = 0.42, power = 0.82) and there was also a significant Tests × Treatment interaction effect (p = 0.003, Eta2 = 0.52, power = 0.96). There were no other significant effects (ps > 0.1, Eta2 = 0.18 – 0.31, power = 0.29 – 0.59). The results from the univariate F tests concerning Tests, Tests × Treatment interaction, and Diagnosis are given below. For means and standard deviations, see Table 1.
Table 1. Means and Standard Deviations for Subjective Pain Before and After 12 or 33 Flotation Treatments
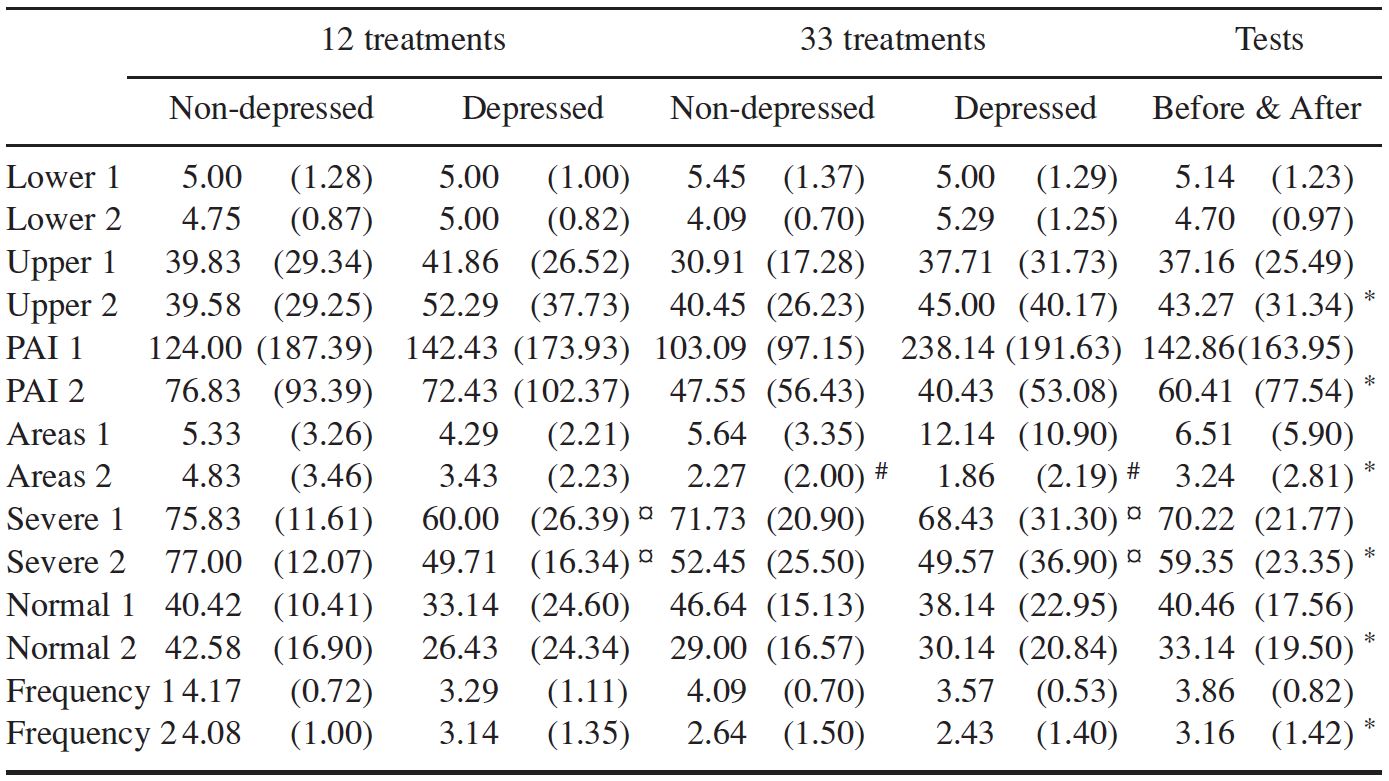
Note: Lower Pain Threshold (Lower), Upper Pain Threshold (Upper), the PAI, Number of Comprehensive Pain Areas (Areas), Most Severe Pain Intensity (Severe), Normal Pain Intensity (Normal) and Pain Frequency (Frequency) (Tests 1-2) in Regard to Treatment (12 Treatments, 33 Treatments) and Diagnosis (Non-Depressed, Depressed).
Significant effects for Tests (p < 0.05) are indicated in the After conditions with *. Significant interaction effect for Tests × Treatment (p < 0.05) is indicated in the 33 treatments and After conditions with #. Significant effect for Diagnosis (p < 0.05) is indicated in the Depressed condition (1-2) with ¤.
Pain thresholds There were no significant effects for lower pain threshold (ps > 0.05) but there was a significant effect for upper pain threshold in regard to Tests [F(1, 33) = 4.93, p = 0.033], where further analysis showed that the participants enhanced their capacity to endure pain. There were no other significant effects (ps > 0.05).
Pain Area Inventory The analyses yielded a significant difference for Tests [ F(1, 33) = 21.19, p < 0.001], and a descriptive analysis showed that pain assessed with the PAI was reduced after the flotation sessions. There were no other significant effects (ps > 0.05).
The number of comprehensive pain areas The analyses yielded a significant effect for Tests [F(1, 33) = 20.00, p < 0.001], and a descriptive analysis showed that the number of comprehensive pain areas diminished during the flotation sessions. There was also a significant Tests × Treatment interaction effect [F(1, 33) = 13.42, p < 0.001], and further analysis (pair-samples t tests, 5 % level) showed that there was no significant difference in regard to the number of comprehensive pain areas after 12 flotation-REST treatments (before: M = 4.95, SD = 2.90; after: M = 4.32, SD = 3.07) but there was such a significant effect after 33 treatments (before: M = 8.17, SD = 7.69; after: M = 2.11, SD = 2.03). There was no significant effect for Diagnosis (p > 0.05).
The most severe pain intensity The analyses yielded a significant difference for Tests [F(1, 33) = 9.26, p = 0.005], and a descriptive analysis showed that the most severe pain intensity was reduced after the flotation sessions. There were no other significant effects (ps > 0.05). In addition, there was a significant effect for Diagnosis [F(1, 33) = 4.09, p = 0.050], suggesting that participants without burn-out depression experienced higher severe pain intensity as compared to participants with burn-out depression. There was no significant Tests × Treatment interaction effect (p > 0.05).
Normal pain intensity The analyses yielded a significant difference for Tests [F(1, 33) = 5.33, p = 0.027], and a descriptive analysis showed that normal pain intensity diminished after the flotation sessions. There were no other significant effects (ps > 0.05).
Pain frequency. The analyses yielded a significant difference for Tests [F(1, 33) = 8.72, p = 0.006], and a descriptive analysis showed that the pain frequency diminished from more or less daily to weekly after the flotation sessions. There were no other significant effects (ps > 0.05).
Stress Related Psychological Variables
A three-way mixed Pillais’ MANOVA was carried out with Tests (before, after) as the within-subjects factor and Treatment (12 treatments, 33 treatments) and Diagnosis (nonburn-out patients, burn-out patients) as between-subjects factors. Dependent variables were the psychological variables, that is, stress (SE), energy (SE), anxiety (HAD) and depression (HAD), dispositional optimism (LOT), positive affectivity (PANAS), negative affectivity (PANAS), and sleep quality (VAS-scale). The analysis yielded significant effects for Tests (p < 0.001, Eta2 = 0.70, power > 0.99), for Diagnosis (p = 0.048, Eta2 = 0.44, power = 0.77) and there was also a nonsignificant tendency for a Tests × Diagnosis interaction effect (p = 0.056, Eta2 = 0.43, power = 0.75). There were no other significant effects (ps > 0.1, Eta2 = 0.25 – 0.38, power = 0.35 – 0.63). The results from the univariate F tests concerning Tests, Diagnosis and Tests × Diagnosis interaction, are given below. For means and standard deviations, see Table 2.
Table 2. Means and Standard Deviations for Stress-Related Psychological Variables Before and After 12 or 33 Flotation Treatments (Tests 1-2) in Regard to Treatment
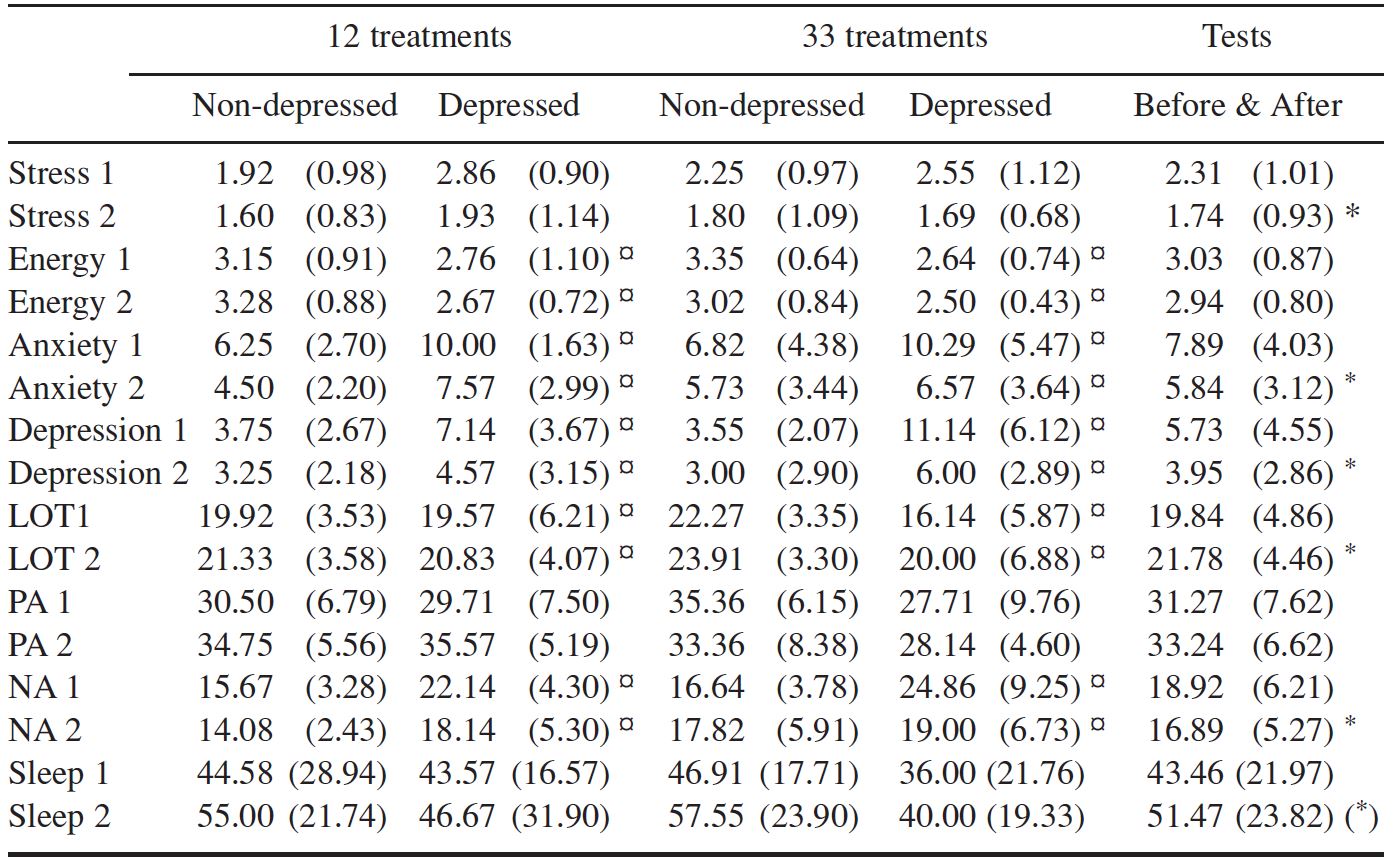
Note: Stress, energy, anxiety, depression, dispositional optimism (LOT), positive affectivity (PA), negative affectivity (NA), and sleep quality (Sleep) (12 treatments, 33 treatments) and Diagnosis (Non-depressed, Depressed)
Significant effects for Tests (p < 0.05) are indicated in the After conditions with *. A nonsignificant trend (p = 0.053) for Tests is indicated with (*). Significant effect for Diagnosis (p < 0.05) is indicated in the Depressed condition (1-2) with ¤.
Stress The analyses yielded a significant difference for Tests [F(1, 33) = 12.19, p = 0.001], and a descriptive analysis showed that stress was reduced after the flotation sessions. There were no other significant effects (ps > 0.05).
Energy The analyses yielded a significant effect for Diagnosis [F(1, 33) = 5.55, p = 0.026], where those participants who did not have a burn-out diagnosis displayed more combined energy compared to those who did have this diagnosis. There were no other significant effects (ps > 0.05).
Anxiety The analyses yielded a significant difference for Tests [F(1, 33) = 20.51, p < 0.001], and a descriptive analysis showed that the anxiety was reduced after the flotation sessions. There was also a significant effect for Diagnosis [F(1, 33) = 6.32, p = 0.017], where further analysis showed that participants without burn-out depression experienced lower anxiety as compared to participants with burn-out depression. Finally, the analysis showed no significant effect for Tests × Diagnosis interaction (p > 0.05).
Depression The analyses yielded a significant difference for Tests [F(1, 33) = 20.61, p < 0.001], and a descriptive analysis showed that depression diminished after the flotation sessions. In addition, there was a significant difference for Diagnosis [F(1, 33) = 11.38, p = 0.002], and a descriptive analysis showed that the participants who did not have the diagnosis of burn-out depression displayed a lower level of depression compared to those who did have the diagnosis. Finally, there was also a significant Tests × Diagnosis interaction effect [F(1, 33) = 11.73, p = 0.002], and further analysis (pair-samples t tests, 5 % level) showed that there was no significant difference in levels of depression before and after the flotation sessions in the nondepressed group (before: M = 3.65, SD = 2.35; after: M = 3.13, SD = 2.49) but there was such a significant effect in the group with patients with burn-out depression (before: M = 9.14, SD = 5.27; after: M = 5.29, SD = 3.00).
Optimism The analyses yielded a significant difference for Tests [F(1, 33) = 13.33, p < 0.001], and a descriptive analysis indicated that optimism increased after the flotation sessions. There was also a significant effect for Diagnosis [F(1, 33) = 4.35, p = 0.045], and a descriptive analysis showed that the participants without burn-out depression exhibited greater optimism compared to those with the diagnosis. Finally, the analysis showed no significant effect for Tests × Diagnosis interaction (p > 0.05).
Positive affectivity There were no significant effects for positive affectivity in regard to those dimensions which the omnibus analysis found significant, that is, Tests, Diagnosis and Tests × Diagnosis interaction (ps > 0.05).
Negative affectivity The analyses revealed a significant effect for Tests [F(1, 33) = 5.41, p = 0.027], and a descriptive analysis showed that negative affectivity diminished after the flotation sessions. Further, there was a significant difference for Diagnosis [F(1, 33) = 11.96, p = 0.022], and a descriptive analysis showed that the participants without burn-out depression displayed less negative affectivity compared to those with the diagnosis. Finally, there was also a significant Tests × Diagnosis interaction effect [F(1, 33) = 7.27, p = 0.0011], and further analysis (pair-samples t tests, 5 % level) showed that there was no significant difference in levels of negative affectivity before and after the flotation sessions in the non-depressed group (before: M = 16.13, SD = 3.48; after: M = 15.87, SD = 4.74) but there was such a significant effect in the group with patients with burn-out depression (before: M = 23.50, SD = 7.07; after: M = 18.57, SD = 5.84).
Sleep quality There were no significant effects for sleep quality (ps > 0.05), even though a nonsignificant trend (p = 0.053) indicated that the patients improved their sleep after the flotation sessions.
Blood Pressure
Statistical analyses were conducted using three-way split-plot ANOVAs with Tests (before, after) as the within-subjects factor and Treatment (12 treatments, 33 treatments) and Diagnosis (nonburn-out patients, burn-out patients) as between-subjects factors and with blood pressure (mmHg) as dependent variables. For means and standard deviations, see Table 3.
Table 3. Means and Standard Deviations for Blood Pressure
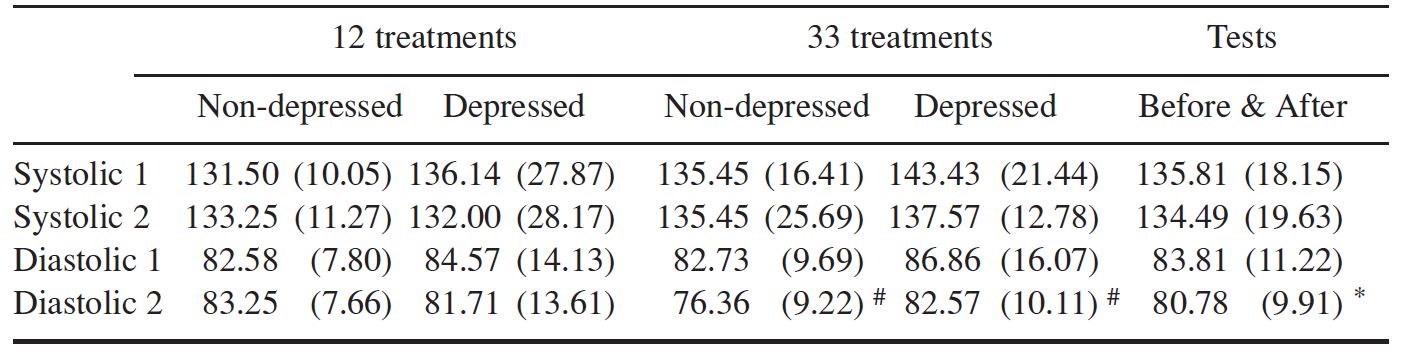
Note: Systolic and diastolic before and after 12 or 33 Flotation Treatments (Tests 1-2) in regard to Treatment (12 treatments, 33 treatments) and Diagnosis (Non-depressed, Depressed)
Significant effect for Tests (p < 0.05) is indicated in the After conditions with *. Significant interaction effect for Tests × Treatment (p < 0.05) is indicated in the 33 treatments and After conditions with #.
Blood pressure, systolic The analyses yielded no significant effects for Treatment, Tests, Diagnosis or their interactions (ps > 0.05).
Blood pressure, diastolic The analyses yielded a significant difference for Tests [F(1, 33) = 10.68, p = 0.003], and a descriptive analysis showed that the diastolic blood pressure diminished during the treatment period. There was also a significant Tests × Treatment interaction effect [F(1, 33) = 4.64, p = 0.039], and further analysis (pair-samples t tests, 5 % level) showed that there was no significant difference in regard to the diastolic blood pressure after 12 flotation-REST treatments (before: M = 83.32, SD = 10.23; after: M = 82.68, SD = 9.91) but there was such a significant effect after 33 treatments (before: M = 84.33, SD = 12.27; after: M = 78.78, SD = 9.79). There were no other significant effects (ps > 0.05).
Discussion
The aim of this study was to investigate whether or not 33 flotation sessions would be more effective than 12 sessions. The results after 12 sessions were in line with recent studies (Bood et al., 2005; 2006) but surprisingly enough the results indicated no, or small, differences between the two programs in regard to treatment effects. Certainly the analyses for subjective pain showed that the number of comprehensive pain areas significantly lowered after 33 flotation sessions but not after 12 sessions. However, for upper pain threshold, the PAI, most severe pain intensity, normal pain intensity, and pain frequency, 12 sessions were enough to get considerable improvements and no further improvements were noticed after 33 sessions. A similar pattern was observed concerning the stress-related psychological variables. After 12 flotation sessions experienced stress had decreased with 25% of participants, anxiety with 26%, negative affectivity with 11%, and depression with 32%, while dispositional optimism increased with 10% and sleep quality with 18% but there were no further improvements after 33 flotation sessions. Concerning measurements for blood pressure, earlier findings have indicated conflicting results after 12 sessions (Bood et al., 2005; 2006). In the present study no effects were observed after 12 flotation sessions, but there was a significant effect for diastolic blood pressure after 33 sessions.
As expected the patients with the diagnosis of burn-out depression had higher values on depression and negative affectivity than did patients without such a diagnosis. Consequently, it was the depressed patients who made the significant improvements in regard to depression and negative affectivity. There were no other interaction effects between Tests and Diagnosis but the patients with burn-out depression had lower values on energy and optimism and higher values on anxiety than did patients without such a diagnosis.
Even though the present study indicated that for several stress-related variables 12 flotation sessions seem sufficient, it should be noted that this is not an over-all recommendation. Firstly there is always the individual factor to consider; patients have different backgrounds and personalities which will influence the treatments. Secondly, ongoing investigations with patients with fibromyalgia or whiplash problems strongly indicate a need for longer treatment programs. Thirdly, an important conclusion that can be drawn from the present study would be the urgency of finding suitable complements to the flotation tank in order for patients with stress-related ailments to make further progress after an initial floating period of about 12 sessions. Programs encouraging a healthier life-style, as well as different combinations with therapy, should probably be considered.
References
Alstergren, P., & Förström, J. (2003). Acute oral pain intensity and pain threshold assessed by intensity matching to pain induced by electrical stimuli. Journal of Orofacial Pain, 17 (2), 151-159.
Benson, H. (1975). The relaxation response. New York: Morrow.
Bood, S. Å., Sundequist, U., Kjellgren, A., Nordström, G., & Norlander, T. (2005). Effects of flotation-REST (Restricted Environmental Stimulation Technique) on stress related muscle pain: What makes the difference in therapy, attention-placebo, or the relaxation response? Pain Research and Management, 10, 201-209.
Bood, S. Å., Sundequist, U., Norlander, T., Nordström, L., Nordenström, K., Kjellgren, A., & Nordström, G. (2006). Eliciting the relaxation response with help of flotation-REST (Restricted Environmental Stimulation Technique) in patients with stress related ailments. International Journal of Stress Management, 13, 154-175.
Kjellberg, A., & Iwanowski, S. (1989). Stress/energi formuläret: Utveckling av en metod för skattning av sinnesstämning i arbetet [The Stress/energy questionnaire: Development of a method for assessment of mood at work]. Solna, Sweden: Arbetsmiljöinstitutet.
Kjellgren, A., Sundequist, U., Norlander, T., & Archer, T. (2001). Effects of flotation-REST on muscle tension pain. Pain Research and Management, 6, 181-189.
Linton, S. J. (1982). Applied relaxation as a method of coping with chronic pain: A therapists guide. Scandinavian Journal of Behavior Therapy, 11, 161-174.
Melzack, R. (2001). Pain and the neuromatrix in the brain. Journal of Dental Education, 65, 1378-1382.
Norlander, T., Kjellgren, A., & Archer, T. (2001). The experience of flotation-REST as a function of setting and previous experience of altered states of consciousness. Imagination Cognition and Personality, 20, 161-178.
Sandlund, E. S., & Norlander, T. (2000). The effects of Thai Chi Chuan relaxation and exercise on stress responses and well-being: An overview of research. International Journal of Stress Management, 7, 139-149.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219-247.
van Dierendonck, D., & te Nijenhuis, J. (2005) Flotation Restricted Environmental Stimulation Therapy (REST) as a stress management tool for enhancing well-being and performance: A meta-analysis. Psychology & Health, 20, 405-412.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect. The PANAS scale. Journal of Personality and Social Psychology, 54, 1063-1070.
Zigmond, A. S., & Snaith R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-370.
Alstergren, P., & Förström, J. (2003). Acute oral pain intensity and pain threshold assessed by intensity matching to pain induced by electrical stimuli. Journal of Orofacial Pain, 17 (2), 151-159.
Benson, H. (1975). The relaxation response. New York: Morrow.
Bood, S. Å., Sundequist, U., Kjellgren, A., Nordström, G., & Norlander, T. (2005). Effects of flotation-REST (Restricted Environmental Stimulation Technique) on stress related muscle pain: What makes the difference in therapy, attention-placebo, or the relaxation response? Pain Research and Management, 10, 201-209.
Bood, S. Å., Sundequist, U., Norlander, T., Nordström, L., Nordenström, K., Kjellgren, A., & Nordström, G. (2006). Eliciting the relaxation response with help of flotation-REST (Restricted Environmental Stimulation Technique) in patients with stress related ailments. International Journal of Stress Management, 13, 154-175.
Kjellberg, A., & Iwanowski, S. (1989). Stress/energi formuläret: Utveckling av en metod för skattning av sinnesstämning i arbetet [The Stress/energy questionnaire: Development of a method for assessment of mood at work]. Solna, Sweden: Arbetsmiljöinstitutet.
Kjellgren, A., Sundequist, U., Norlander, T., & Archer, T. (2001). Effects of flotation-REST on muscle tension pain. Pain Research and Management, 6, 181-189.
Linton, S. J. (1982). Applied relaxation as a method of coping with chronic pain: A therapists guide. Scandinavian Journal of Behavior Therapy, 11, 161-174.
Melzack, R. (2001). Pain and the neuromatrix in the brain. Journal of Dental Education, 65, 1378-1382.
Norlander, T., Kjellgren, A., & Archer, T. (2001). The experience of flotation-REST as a function of setting and previous experience of altered states of consciousness. Imagination Cognition and Personality, 20, 161-178.
Sandlund, E. S., & Norlander, T. (2000). The effects of Thai Chi Chuan relaxation and exercise on stress responses and well-being: An overview of research. International Journal of Stress Management, 7, 139-149.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219-247.
van Dierendonck, D., & te Nijenhuis, J. (2005) Flotation Restricted Environmental Stimulation Therapy (REST) as a stress management tool for enhancing well-being and performance: A meta-analysis. Psychology & Health, 20, 405-412.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect. The PANAS scale. Journal of Personality and Social Psychology, 54, 1063-1070.
Zigmond, A. S., & Snaith R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-370.
Table 1. Means and Standard Deviations for Subjective Pain Before and After 12 or 33 Flotation Treatments
Note: Lower Pain Threshold (Lower), Upper Pain Threshold (Upper), the PAI, Number of Comprehensive Pain Areas (Areas), Most Severe Pain Intensity (Severe), Normal Pain Intensity (Normal) and Pain Frequency (Frequency) (Tests 1-2) in Regard to Treatment (12 Treatments, 33 Treatments) and Diagnosis (Non-Depressed, Depressed).
Significant effects for Tests (p < 0.05) are indicated in the After conditions with *. Significant interaction effect for Tests × Treatment (p < 0.05) is indicated in the 33 treatments and After conditions with #. Significant effect for Diagnosis (p < 0.05) is indicated in the Depressed condition (1-2) with ¤.
Table 2. Means and Standard Deviations for Stress-Related Psychological Variables Before and After 12 or 33 Flotation Treatments (Tests 1-2) in Regard to Treatment
Note: Stress, energy, anxiety, depression, dispositional optimism (LOT), positive affectivity (PA), negative affectivity (NA), and sleep quality (Sleep) (12 treatments, 33 treatments) and Diagnosis (Non-depressed, Depressed)
Significant effects for Tests (p < 0.05) are indicated in the After conditions with *. A nonsignificant trend (p = 0.053) for Tests is indicated with (*). Significant effect for Diagnosis (p < 0.05) is indicated in the Depressed condition (1-2) with ¤.
Table 3. Means and Standard Deviations for Blood Pressure
Note: Systolic and diastolic before and after 12 or 33 Flotation Treatments (Tests 1-2) in regard to Treatment (12 treatments, 33 treatments) and Diagnosis (Non-depressed, Depressed)
Significant effect for Tests (p < 0.05) is indicated in the After conditions with *. Significant interaction effect for Tests × Treatment (p < 0.05) is indicated in the 33 treatments and After conditions with #.
The study was approved by the Ethical Board on Experimentation on Human Subjects (Forskningse- tikkommitté
n) at Ö
rebro Academic Hospital
Ö
rebro
Sweden.
The study was supported by grants from the County Council (Landstinget) in Vä
rmland (LiV)
Sweden.
Appreciation is due to reviewers including
Trevor Archer
PhD
Department of Psychology
Gö
teborg University
Box 100
405 30 Goteborg
Sweden
Jan te Nijenhuis
Self-employed scientific consultant
Amsterdam
The Netherlands
[email protected]">[email protected] and anonymous reviewers.